Meridian: Measuring Biology As It Changes
Much of clinical medicine runs on categorical scales. These instruments—many designed decades ago to classify populations, not track individuals—constitute the default measurement protocol for disease progression across dozens of specialties. They are applied episodically: a snapshot every few weeks in a disease that does not pause. Between snapshots, biology progresses, baselines shift, and raters change. Such fragmentation introduces irreducible noise masking true markers of biological change.
Tackling metric bluntness and fragmentation matters beyond any single rating protocol in isolation; the resolution of clinical labels propagates into every downstream system that inherits it. When a machine learning model is trained to predict disease progression, it is trained against these ground truths. A model trained on noisy clinical labels learns noise––a suboptimal use of compute, and therefore capital. Coarse clinical scales invariably set the ceiling for the clinical validity encoded in latent maps.
The data to resolve clinical fragmentation already exists: kinematics, spirometry, blood panels, vital signs, wearable streams, imaging, genomics. What has been missing is more foundational: a scalable and interpretable measurement layer––a principled method for establishing where a patient or population started, quantifying whether the system has meaningfully departed from that point, and decomposing what drove the departure in a way that is interpretable, auditable, and reproducible.
Meridian is that method.
Its mathematical heritage is specific. The problem of measuring change under noise, at speed, from incomplete and indirect observations, is one that particle physics solved a long time ago. At the Large Hadron Collider, particle showers produced in high-energy beam interactions traverse layers of detectors, each recording a time-slice imprint of the energy, and, therefore, information, flow. The trajectory is never observed directly. It is inferred from geometry: from the spatial and temporal relationships between those partial measurements, and from what the structure of the detector and the physics of the interaction allow. The mathematics that recovers a particle's true path from fragmented detector responses is, at its core, the mathematics of measuring change across a space-time trajectory in a system you cannot observe whole.
Biological data presents the same structure. A patient is measured at intervals, through instruments that capture fragments of a deeper physiological state. The signal is indirect, partial, noisy, irregularly sampled. The state itself is latent. What the clinician needs is not more data but a principled way to establish a reference baseline state, track departure from it, and decompose what drove the change. This is not an analogy. It is the same mathematical problem, and it admits the same class of solutions.
Meridian is a mathematical framework for measuring biological change. Given any physiological signal, in any modality, it establishes a reference coordinate and computes whether the system has drifted from it in a way that is sustained and explained by physiological drivers, rather than noise. It identifies which dimensions of the signal carry the change and which do not. It decomposes the structure of that change so that the answer is not simply "something moved" but "this is what moved, by how much, and with what confidence." Notably, there is no AI involved. The framework operates on the geometry of the data itself. Its outputs are fully traceable. We built a principled metric of biological change that will pass the test of time.
The same framework operates cross-sectionally, on a single snapshot, and longitudinally, across seconds, days, months or years of follow-up. It operates on small datasets where deep learning cannot be supported and on large ones where it can be composed with the higher layers of the measurement stack. It admits any data modality. It does not need to be re-engineered per disease, per sensor, or per indication.
To date it has been applied across more than 7 million individuals, 30 clinical conditions, and counting. The mathematics does not change between them. The data does. That generality is not a design aspiration. It is a mathematical property of the framework, and it is what makes the results that follow possible.
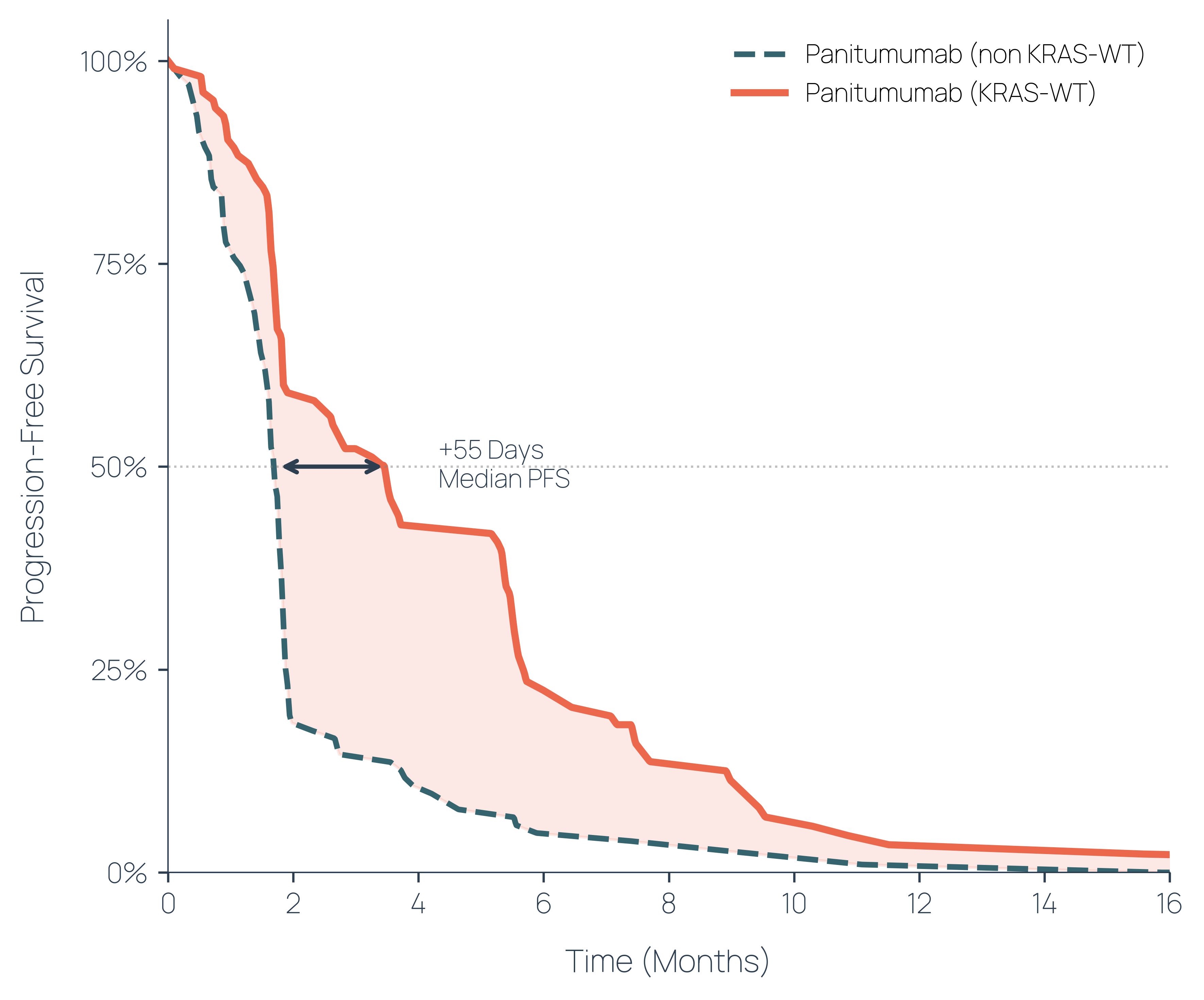
In metastatic colorectal cancer, a targeted therapy called panitumumab showed modest efficacy in its Phase 3 trial: a median improvement of five days in progression-free survival across the full population. Progression-free survival measures how long a patient lives without their disease worsening. Strong responders existed, but they were hidden by the heterogeneity of a mixed population. We applied Meridian to routine baseline data from 171 patients across seven clinical features, without specifying which feature to examine. The framework identified the axis of maximum treatment-response heterogeneity and isolated the responsive subgroup. In that subgroup, the measured treatment effect was eleven times stronger: 55 days of additional progression-free survival. The biomarker the framework recovered, KRAS wild-type status, subsequently became the standard of care for panitumumab prescribing. The platform found it from the data alone, without the biological hypothesis that guided its original discovery.
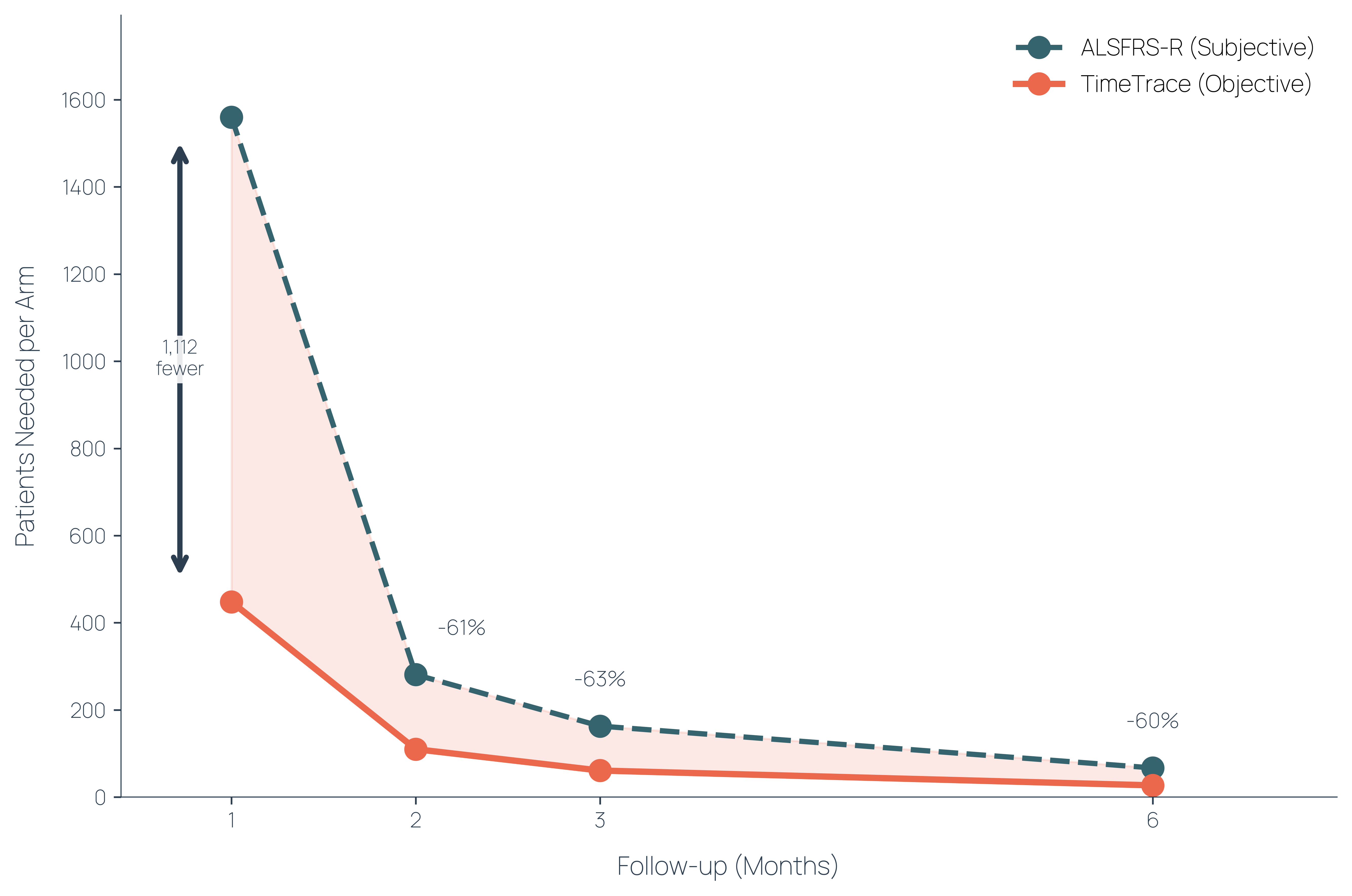
In amyotrophic lateral sclerosis (motor neuron disease), disease progression is typically measured using a clinician-administered questionnaire that scores functional ability across twelve activities. It is subjective, coarse, and often requires six months of follow-up before meaningful change becomes detectable. We applied Meridian to longitudinal spirometry data, a measure of breathing capacity, from 1,643 patients across pooled Phase II and III trials. The framework identified the most sensitive respiratory progression axis and detected statistically meaningful change at one month. Six times earlier. For equivalent statistical power, this translates to 70% fewer patients per trial arm. The same disease, the same patients, the same data. A different measurement.
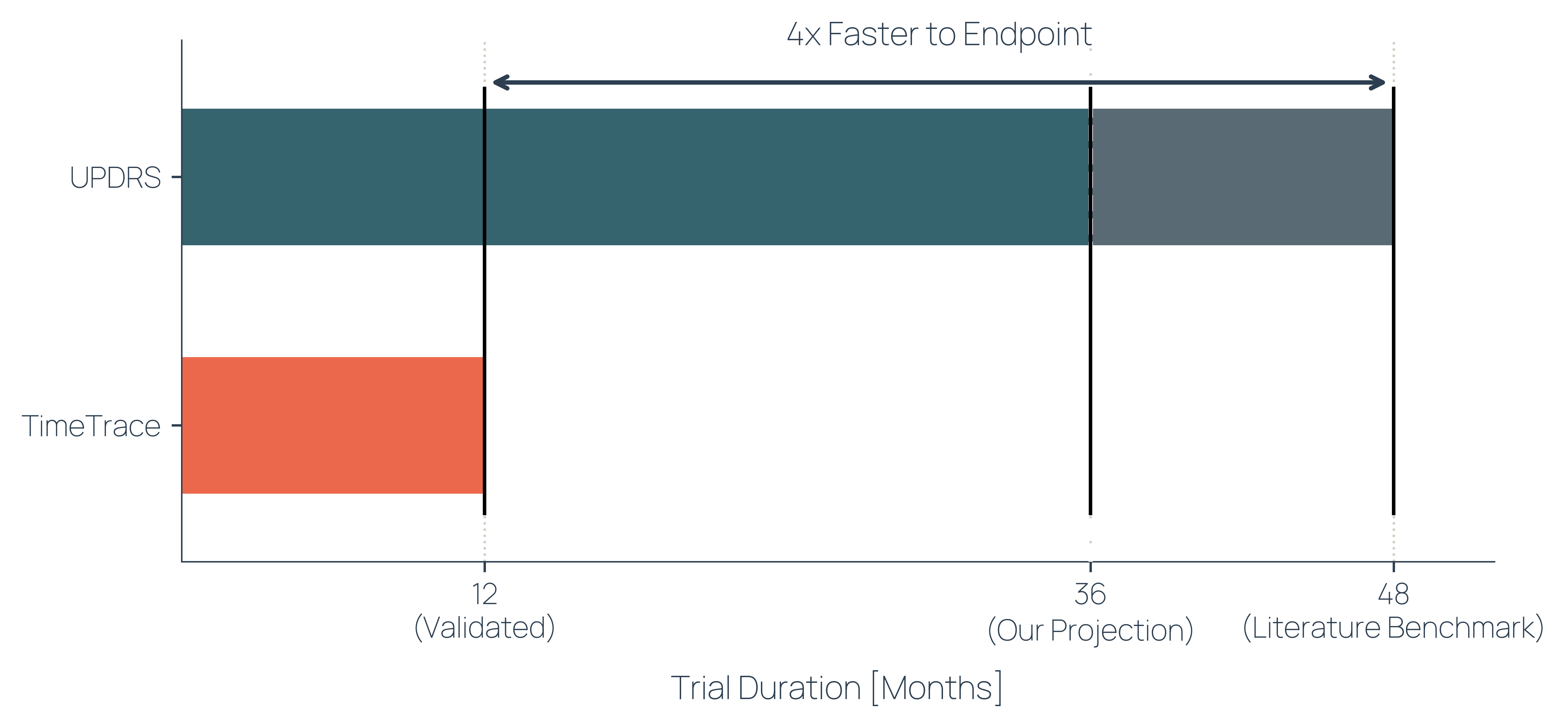
In Parkinson's disease, the gold standard for measuring progression is the UPDRS, a clinical rating scale introduced in the 1980s in which a neurologist scores a patient's movement, tremor, rigidity, and daily function through observation and interview. It remains the primary endpoint in nearly every Parkinson's trial. It is subjective, noisy, and detecting treatment effects typically requires three to four years of follow-up. We applied Meridian to kinematic data: the movement patterns captured by wearable sensors during routine clinical tasks. The framework detected progression at twelve months. No new data collection. No new instruments. Four times faster to endpoint. This is where the framework was born, in the movement signatures of neurodegenerative disease, and it is where its sensitivity remains sharpest.
Three diseases. Three data modalities. Three clinical contexts in which the standard instruments require years or large populations to see what the mathematics resolves in days, weeks or months. The framework did not change between them. This is what it means to own the measurement layer rather than build bespoke analytics per indication: generalisability by way of foundational mathematical grounding; shorter time-to-signal by way of noise reduction; replacement of categorical scores with a single calibrated statistical engine.
This is the simplest way to describe what Meridian does: it makes biological change measurable where it was previously beneath the resolution of the instrument. Everything that follows from better measurement, earlier detection, smaller trials, subgroup identification, continuous monitoring, endpoints that resolve treatment effect where existing scales cannot, is a consequence of that single capability. Meridian sits across the layers of the measurement stack. It draws on the mathematical foundation, composes with learned representations where they are available, and produces the measurement outputs on which every downstream decision depends.
It is the component from which the others take their coordinates. Across diseases, modalities, and scales.
Please cite this work as:
TimeTrace Labs. Meridian: Measuring Biology As It Changes. TimeTrace Labs Blog, April 2026.
BibTeX:
@article{timetrace2026meridian,
author = {{TimeTrace Labs}},
title = {Meridian: Measuring Biology As It Changes},
journal = {TimeTrace Labs Blog},
year = {2026},
url = {https://www.timetracelabs.com/blog/meridian}
}